EMG Nerve Conduction Study Test Results Jamie Boyle Guillain Barre Syndrome
I saw Jamie Boyle, a 41 year old gentleman, in the Electrodiagnostic Lab at the Dr. Everett Chalmers Regional Hospital on October 23, 2019 for an EMG nerve conduction study. As you know, he had progressive rapid muscle weakness in his extremities which started on August 2nd, 2019. He reported having an episode of gastroenteritis with acute diarrhea which lasted around one week before his muscle weakness. He was admitted to the Dr. Georges Dumont Hospital and since the muscle weakness rapidly progressed, he was intubated and transferred to the ICU. He was put on mechanical ventilation on August 3rd, 2019. Guillain Barre Syndrome was diagnosed by neurology there and he received intravenous immunoglobulin to treat this condition.
Subsequently, he did develop a few nosocomial complications such as urosepsis, ileus, acute renal failure, pneumonia, bronchitis and tracheitis. He was eventually transferred to The Stan Cassidy Rehabilitation Centre for rehabilitation. He received two more IVIG courses of treatment, 5 days each time. He says he improved some.
His past medical history is positive for hypertension. Otherwise, he was a fairly healthy man.
PHYSICAL EXAMINATION
Mental status was unremarkable in routine interview. Language was normal. Extraocular movement was normal. No ptosis. No facial palsy. Tongue protruded in the midline without fasciculation or atrophy. He had severe flaccid quadriplegia. In the upper extremity, proximal muscle strength was 1-2/5 and distal was 1/5. In the lower extremities, proximal muscle strength was 2/5 and distal was 1/5. Deep tendon reflexes were absent. He had mild interosseous muscle atrophy.
Electrophysiologic study was requested for further evaluation. EMG nerve conduction study.
NERVE CONDUCTION STUDIES:
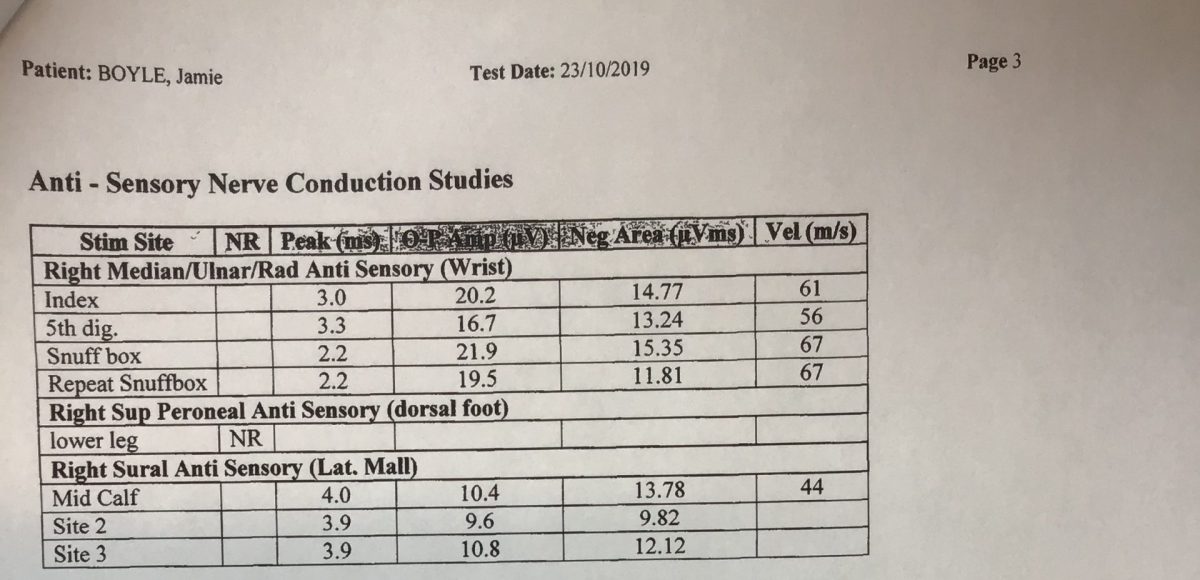
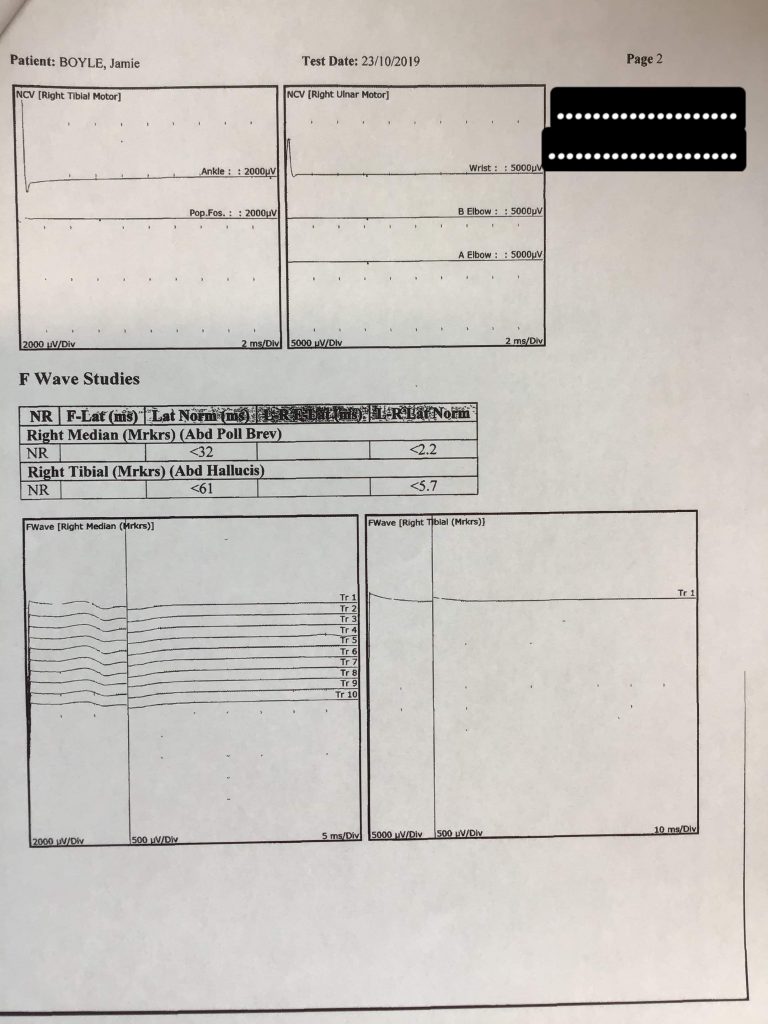
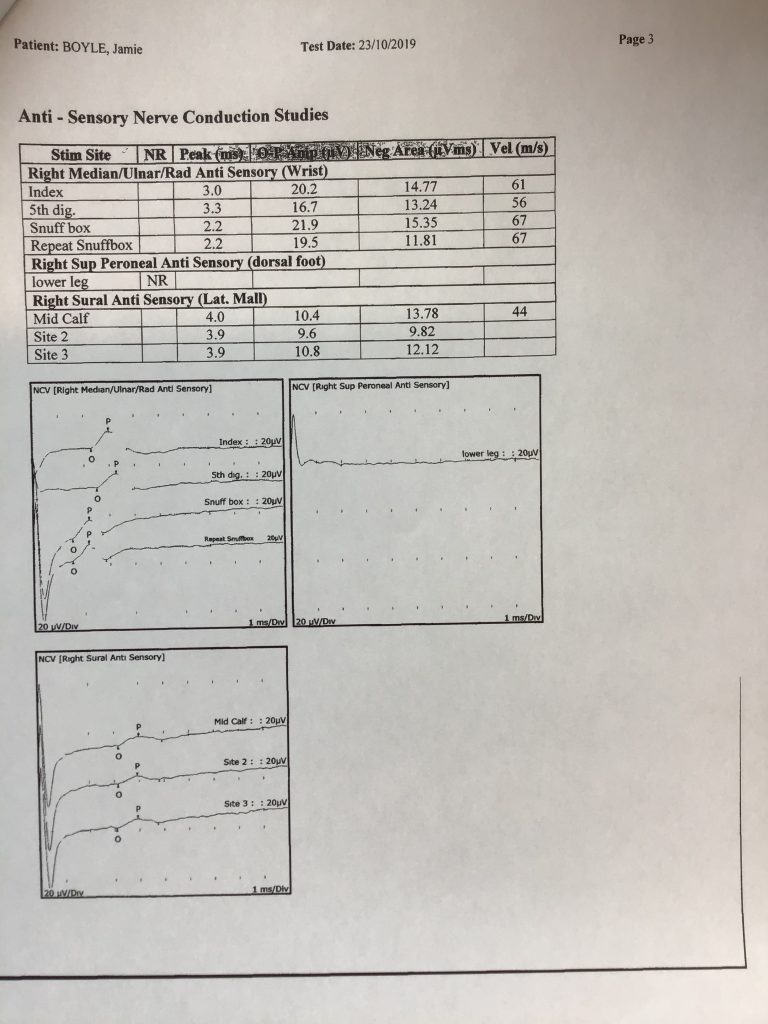
In the right upper extremity, median motor distal latency was 4.5 msec with amplitude reduced significantly at 0.4 millivolts. Conduction velocity was reduced at 34 m/s. The amplitude of the median nerve in distal stimuli was 0.4 millivolts and in proximal stimuli was 0.2 millivolts. Although as a definition there is 50% reduction in the amplitude of motor nerves in the proximal stimuli, it could be impacted by very low amplitude and we cannot determine the typical conduction block in the median nerve. Ulnar motor evaluation was nonresponsive. Median sensory peak latency was 3 msec, ulnar was 3.3 and radial was 2.2 msec with normal amplitude.
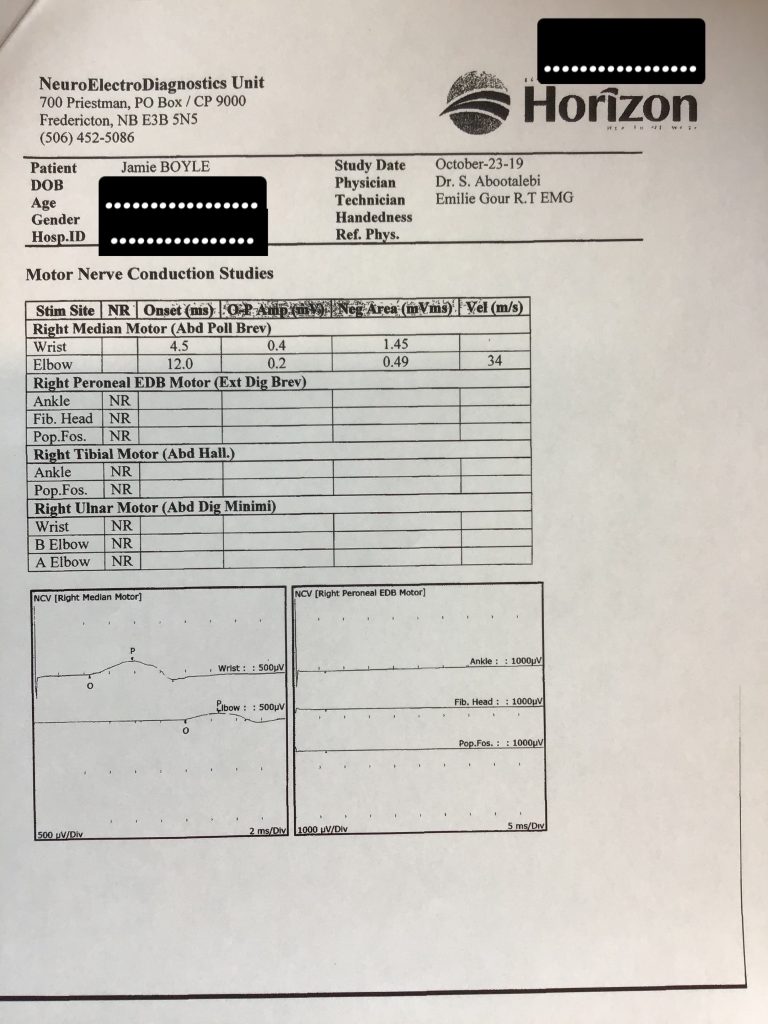
In the right lower extremity, peroneal motor and tibial were not obtainable. Superficial peroneal sensory was not obtainable. Sural sensory peak latency was 4 msec with amplitude at 10 microvolts.
EMG STUDIES:
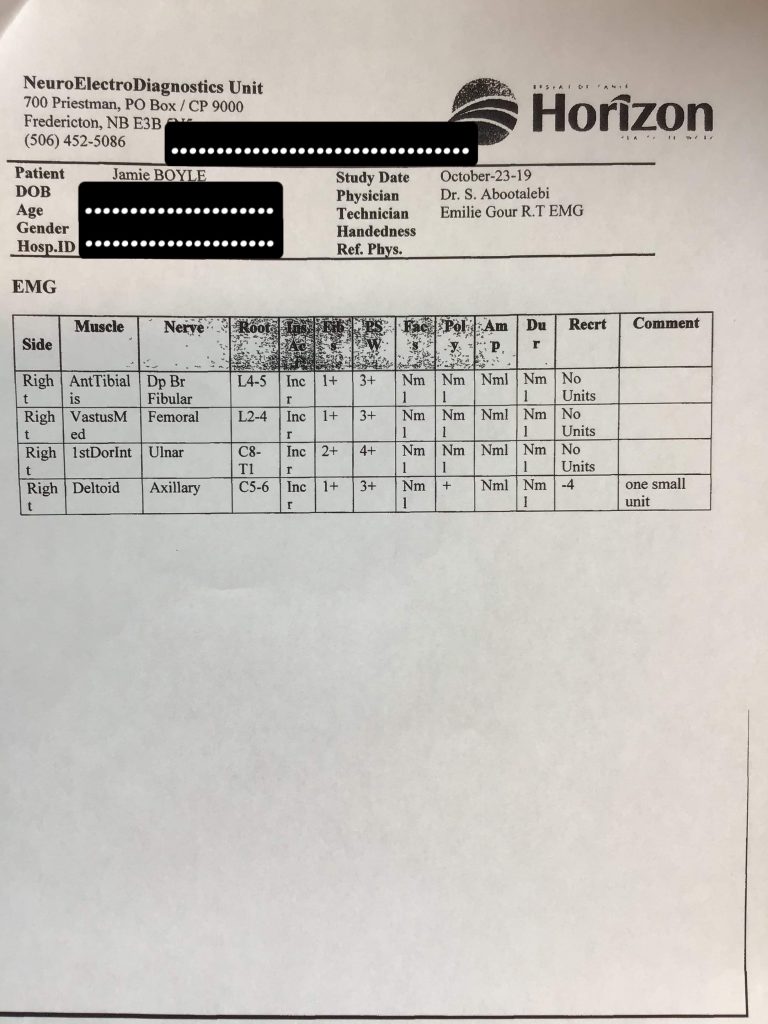
A concentric needle EMG was performed on the right anterior tibialis, vastus medialis, first dorsal interosseous and deltoid muscles. Insertion activity was increased in all the muscles in the exam. There were 3-4+ sharp waves. Only on the deltoid muscle, there was small motor unit involuntary contraction. No motor units were obtained in the other muscles.
IMPRESSION AND RECOMMENDATION:
This is an abnormal Electromyography/nerve conduction study and would be consistent with severe motor demyelinating and axonal type polyneuropathy. Guillain Barre Syndrome should be considered as a cause.
With respect to treatment, he received three courses of IVIG. There is no straight forward and well-known recommendations for such condition. He did not have significant improvement with three courses of IVIG. He has severe weakness in all muscles in the upper and lower extremities. He also has significant denervation pattern in the muscles in the exam. With this respect, I recommended we try plasma exchange, five courses, and after plasma exchange, we give him another course of IVIG. After explaining this approach, he agreed to try. Plasma exchange is available in Saint John and the patient likely needs to be transferred to Saint John Regional Hospital for five courses of plasma exchange.
Shahram Abootalebi, MD Neurologist